SANITY AND URBANITY BLOG
If you are an academic, urban designer, planner, health professional or citymaker, and would like to submit a blog, please see submission guidelines.

|
by Matthew Williams, UD/MH Fellow An inviting city has specific characteristics of its built environment which make us feel good. Its most salient characteristic is its (literally built-in) invitation to stop, observe, mingle, interact, and strengthen our social bonds. The great project of a city is, after all, to bring strangers together. Solitude is necessary for contemplation, reflection, and grounding, but it is the connections which cities make possible – everyday prosaic, romantic, and/or professional - that often generate better versions of ourselves and who we can be as a society. The way we lay out our cities from the micro to the macro determines the nature of the invitation. Do we want to invite more cars? Then build more roads and they’ll surely come. But, isn’t it more lively streets and public spaces that makes us feel alive? Then the city's invitation to us is contingent on one imperative: it must nourish our senses and obey our human scale, not the scale of the automobile. It must give us fine-grained detail, not Brutalist-style monoliths, nor vast swathes of ashphalt for cars and their parking spaces. Tokyo is, for the most part, very inviting. That's why I choose to live here. Contrary to the “Lost in Translation” stereotype, the city is not alienating. Tokyo combines density and detail in walkable human-scaled streets and public spaces. Its detail includes, for example, engaging multiple small-scale signage and displays of blossoms at shop entrances, noren (a printed fabric hanging in restaurant entrances, much like a curtain but with a vertical split to allow patrons to enter) and even ceramic bowls of carp in front of a hairdresser.
Signage and blossoms at a shop entrance and bowl of carp in front of a hair salon, Tokyo There are scattered parking lots, but their propinquity to the rich detail elsewhere renders their sensory impact even more jarring. They are spaces of nothingness and desolation. They don't uplift. They diminish us.  Parking lot, Tokyo Tokyo’s detail can only be perceived because it falls within our ‘social field of vision’ in numerous walkable human-scale streets. That is, within a range of up to 100 metres, our our senses are activated enough to engage meaningfully with our surroundings: to recognize the local okonomiyaki (Japanese seafood pancake) restaurant owner taking a break in his shopfront so as to stop and chat; to smell flowers; to notice the hanging noren printed with vegetables signaling a tempura restaurant inside. Tokyo’s predominant ‘architectural speed’ matches this social field of vision. That is, the architecture and the details amassed around it (the intricate woodwork and bamboo arrangement of the shop entrance and the flowers, signs, menus amassed in front) are at a walking (5km per hour) and cycling speed (average 15-20km per hour), not the speed of the automobile (average 60km per hour). This human mobility speed, and even the cycling speed, is visually stimulating and mentally nourishing because we can sense and engage with its details up close as we walk or cycle. Jan Gehl notes with ringing lucidity: “at its core, walking is a special form of communion between people who share public space as a platform and framework”.
Restaurant owner resting outside his shop, and a noren curtain signaling a vegetable tempura restaurant. Medieval cities configured around central town squares and based on human mobility (architecture at walking speed were designed so people could walk in their daily commercial routines. Who hasn’t beamed at the pleasure of walking in a town square in Italy? Tokyo does this superbly in many of its neighbourhoods. It offers abundant ‘experience space’ in small-scale streets, pocket parks, and informal and formal squares, while its major thoroughfares provide the ‘movement space’ for private automobiles, buses, and trucks. And it has vast ‘movement space’ underground in its ubiquitous labyrinthe subway system, which carries workers, students, and the upper middle class. 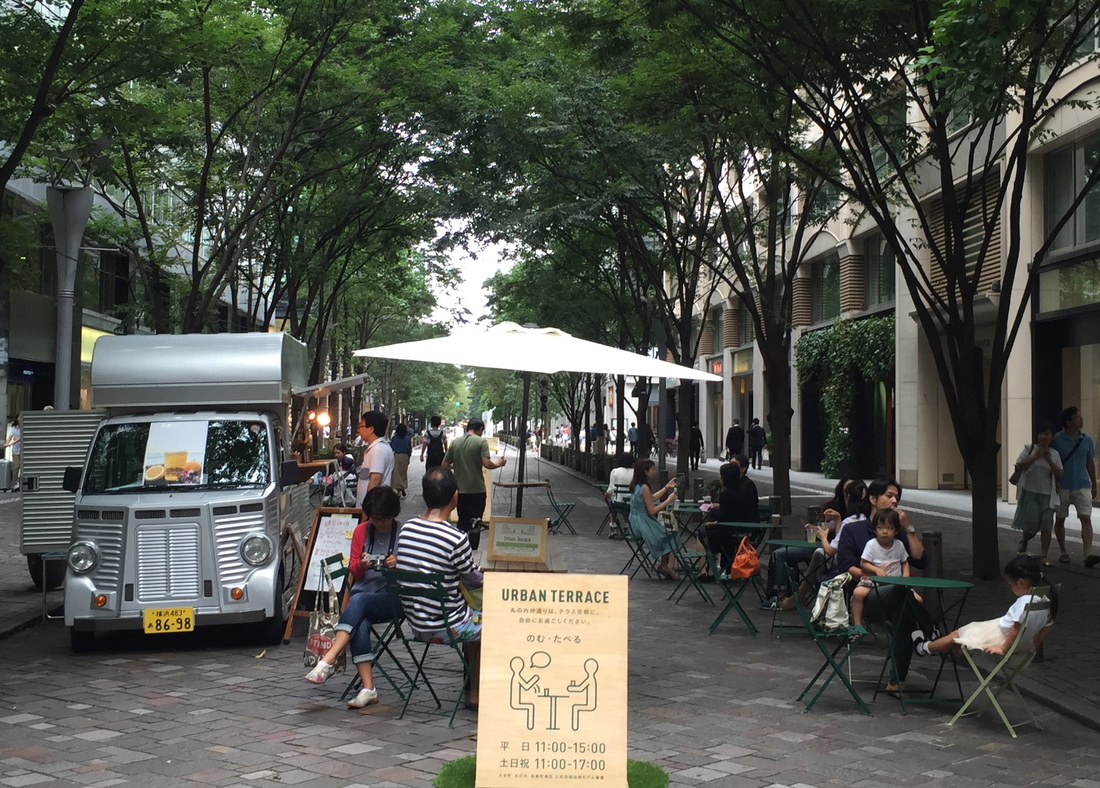 Pocket park, Tokyo This is not the case in many cities where modernism has ignored the ‘life in between buildings’, as Jan Gehl refers to it, and focused on discreet stand-alone buildings intersected by vast networks of roads to accommodate (and ‘invite’) the car invasion of the 20th century. Until that time, as Jane Jacobs opined, city space was primarily ‘experience space’, designed to facilitate social interaction. The automobile upended this paradigm, to the detriment of our social capital and well-being by streamlining city space for the utilitarian purpose of allowing cars fast passage. The automobile radically disrupted human scale because cars take up more space than people, both when driving and parked (a parking lot for 20 to 30 cars and their owners denies a whole metropolitan citizenry a nice-sized town square). In a city of cars, all spatial dimensions increase to accommodate the car’s speed, and we are left with the impoverished experience of the 60 km per hour architecture (‘fast architecture’) of a busy road. Its monochrome blandness ignores human scale precisely because it is not built for humans and their mobility speed. That's the regrettable legacy of the 20th century: we built cities for cars, not for humans.  Cities designed for the spatial dimensions and speed of cars, not people People love to watch other people. They will stop, observe, mingle, sometimes make a new friend, and even occasionally fall in love if there is an appropriate ‘invitation’. The invitation works if it obeys human scale, is designed at a walking or cycling speed, is rich in visual detail such as in Tokyo’s small streets, and pushes cars onto main roads. Tokyo is not perfect but it is a very good touchstone of an ‘inviting’ human-scale city. Monocle magazine ranked Tokyo No. 1 in this years’ annual livability survey. Not undeserving.  The open design invites people to stop and listen to the pianist at a community music centre All photographs by Matthew Williams About the Author
Elika Dadsetan, Social Development Specialist, International Health and Epidemiology Research Center (IHERC), Director of Programs The World Health Organization states: “There is no health without mental health,” which means that in terms of achieving healthy cities, mental health and other supplementary support elements are key. There are many factors for city planners, architects and others to contemplate regarding what a “mentally healthy” environment can look like and how to deliver it, and social-cultural, physical-built, and economic environments all come into play. These factors become particularly important in the context of supporting the mental health of refugees in the city. Mental illnesses are on the rise, and we know that at least one in four people will experience some mental illness in their lives. These numbers are only magnified in communities experiencing distress across the board, such as refugees coming out of Syria. Although it is too soon to discuss impacts of these recent refugee crises, it is very likely that with the highest number of migrants in our modern history, we will see further increases in mental illness in these populations. Due to the stigma and misconceptions around mental illness, people often do not receive adequate medical care. In low and middle-income countries, approximately 80% of people living with mental illness receive no mental health treatment at all, or they use traditional healers that may not deliver effective care. This means they have fewer opportunity to achieve good health, reducing their chances to become involved in projects that may be able to help them out of poverty, or at least be able to afford the health care they require, creating a further vicious circle of poverty and mental illness. Thus, we cannot ignore mental health as a key determinant of health in urban contexts. We have to include mental health as part of the discussions about how we can encourage “healthy cities” for the sake of children and adults alike. Taking into consideration what types of positive support systems are needed for refugee populations, and others living in poverty, is key to “city” planning. Children's mental health can be particularly impacted by growing up in slums and refugee camps. First, we know that poverty is inextricably linked with mental illness, and can create and maintain a vicious cycle. People who live in urban poverty are at particular risk of mental illness, and those who are mentally ill are at a greater risk of social discrimination and exclusion; without healthy support systems, these people are more likely to experience extreme poverty.  Syrian refugee siblings in front of their tent. In the background there’s a photo of a fancy house- the boy explained that this is their dream house. Photograph by Ralph Baydoun, World Vision Lebanon. Living in cities increases the risk of developing certain mental illnesses, and for refugees living in urban poverty, these risks are often exacerbated because their living environments are often inherently stressful. For example, we know that children may have increased exposure to domestic and sexual violence, they may be more likely to worry about economic hardships, including child labor and child marriage, and children in these settings may experience greater levels of neglect or lack of parental engagement, since parents often have to spend time away from the home to earn money. We also see greater social isolation in urban slums, including refugee camps - both informal tented settlements or otherwise, and as such, increased risks for children to become involved in substance abuse, violence, sexual exploitation, and other risky behaviors and experiences. Furthermore, these children's adult caregivers are also at increased risk of developing mental illnesses - and this is a further risk factor for children's mental health. We know that suicide is amongst the top three causes of death for those of child-bearing age (15-44 year olds). The old “village” life that refugee children may be used to - and the care associated with it - may not be as prominent in their new lives.  Pictures of Syrian refugees during winter season in Lebanon. Photograph by Ralph Baydoun, World Vision Lebanon. Stress is, of course, a normal brain response to threat - but when it occurs constantly, stress can cause the structure of the brain to change. Research has shown that the amygdala (an area of the brain that regulates emotions like anxiety and fear) shows higher activation levels in healthy individuals living in large cities than in healthy counterparts living in rural regions. Our brains start developing before we are born and continue up through the age of 23 or 24, so consistent stress associated with living in urban areas may literally alter young people's brain structure, which may lead to increased stress levels, anxiety, life-long hyperactivity, and greater vulnerability to various adult mental illnesses. Children with higher stress or childhood disorders are also less likely to do well at school, which affects their education and work opportunities. This challenge is magnified for refugee children, at least half of whom are out of school (at least 3.4 million refugee children), which causes further challenges, particularly when they are required to work instead, or get married at a young age. Strategies for designing living environments that promote good mental health for refugees Creating safer public spaces through rebuilding community social networks, strategically improving the built environment, and securing economic opportunities can help change the narrative and help develop resiliency and rebuild the dignity of refugees' communities. The social/community environment When planning the design of living environments for refugees, there needs to be consideration around building capacity (human resources and otherwise) within the communities to capture the needs of individuals with distress. Utilizing experts and leadership from the community to develop strategies that are culturally relevant, appropriate, and effective, needs to be considered. Taking cultural contexts into consideration to ensure appropriate spaces is key. Organizing and promoting regular positive community activities, while providing a voice of power to the community, can help rebuild community social networks, and help redefine the narratives associated with the community. Communities also need to be able to restore a connection to their home countries, and help rebuild a sense of cultural identity, which has been shown to have a positive impact on mental health outcomes. Some of the most successful youth development, violence prevention, and health promotion programs build on existing community assets, and are dependent on community members and organizations that connect individuals to a supportive community. In communities where organizational infrastructure and capacity is lacking or absent, violence and trauma have a more profound impact on individuals and communities. Thus, more effort needs to be made to create social cohesion between the host communities and refugee communities, assuming the host communities have that missing capacity. Churches and spiritual leaders can fulfill some of these roles in many communities, but a healthy community has multiple entry points, including businesses, civic organizations, social organizations, schools, and youth-driven organizations that can contribute to the social and cultural environment that promotes positive relationships, social norms, behaviors, and activities within a community. The physical/built environment Reducing deterioration, and creating space for positive interaction are the most important physical/built environment priorities to support mental health. This may include reclaiming public space to be appealing to residents, reflect their community culture, and become a source of pride that can contribute to a sense of community worth and be supportive of healing. The systematic disinvestment and neglect of poor inner city communities has been a part of the structural violence that has produced community trauma over the last half century in the US, and other western societies. This is only exacerbated in communities that are hosting refugees. Thus, there is a need to focus on improving and maintaining roads, buildings, parks, transportation, and other public services so that they are transformed from sources of toxic stress, into an environment that encourages positive social interaction and relationships. A great example of such an attempt is in Colombia with the various social development projects set up in Medellin. Additionally, parks, playgrounds, and other recreational facilities provide critical opportunities for engaging in physical activity and gathering with neighbors, and especially in order to relieve stress. Their absence undermines community health, mental health and quality of life. Thus, these facilities not only normalizes daily life in the communities, but can serve as safe spaces for youth to gather and socialize, while engaging in physical activity. The economic environment Lastly, strategies to improve economic opportunities for youth and adults in these neighborhoods are critical to the success of healing from community trauma, improving community health and wellness, and resisting the pressures of additional dislocation. Actual workforce development strategies that improve employment skills, capacity, and readiness of community members, while linking them to job opportunities with a living wage is critical. This also helps avoid idle youth in refugee camps being recruited for armed forces, early marriage, or child labor activities. These strategies must be multi-sectoral, focusing on different segments of communities, including strategies to increase the proportion of young people and adults who attend primary, secondary and tertiary (including vocational) education, and undertake job training and placement. Planners must ensure that the infrastructure for people to access these opportunities is available. It would be helpful to institute restorative justice programs that shift the norms around conflict resolution and healing circles to, amongst other outcomes, support people to stay on paths to pursue educational and economic opportunities  Syrian refugees creating their own comfort zones. Photograph by Ralph Baydoun, World Vision Lebanon. What would help Mental health is not always talked about and fully documented in refugee populations; we need more documentation of the extent of the challenge, and more research on the most effective interventions. But for urban planners and designers, there is a need for increased capacity to recognize the needs of these populations: planning consultations with the communities are important - and should include people with mental health problems, and mental health and wellbeing promotion (including opportunities for play) should be actively built into future developments. About the Author
by Layla McCay, UD/MH Director An important new report on urban design and mental health, Urban Sanity: Understanding Urban Mental Health Impacts and How to Create Saner, Happier Cities, has just been published by the Victoria Transport Institute in Canada. The report evaluates the evidence that links urban design and mental health, and uses these specific links to propose policy recommendations. The report author, Todd Litman, asserts that cities generally provide good opportunities for people to thrive - yet research tells us that people who live in cities have an increased risk of psychosis, mood disorders, cocaine and heroin addiction and unhappiness (though a lower risk of dementia, alcohol abuse and suicide) compared to rural dwellers. Why? And what can we do about it? The premise of the report is that urban living in itself does not cause mental disorders or even make people unhappy - rather, city life seems to be associated with increased mental health problems for two principal reasons:
The report identifies factors that are particularly associated with the increased risk of mental illness in the city:
Design and Policy recommendations from the report The report makes specific design and policy recommendations to address the urban risk factors for mental illness identified in the report, replicated here: Targeted social service: Recognize that cities tend to attract people with elevated mental illness risks, and provide appropriate mental health, housing and substance abuse treatment services. Affordability: Improve affordable urban housing and transportation options (walking, cycling, public transit, taxi, etc.) to reduce residents’ financial stress. Independent mobility: Provide independent mobility options for diverse community members, including those who are poor, have disabilities or impairments, adolescents or seniors. Pro-social places: Create public spaces that promote community and encourage positive interactions among residents. Involve residents in creating public places and activities that meet their needs. Community safety: Create communities that minimize urban dangers including traffic, crime and harassment, and pollution exposure. This can involve traffic safety programs, crime prevention though environmental design, appropriate lighting, passive surveillance by nearby residents and bypassers, and other community safety programs. Design for physical activity: Integrate physical activity by providing good walking and cycling conditions, high quality public transit, compact and mixed neighborhoods, local parks and recreational facilities, plus appropriate community sports and recreation programs. Pollution reductions: Implement noise, air, light and toxic pollution reduction programs. Greenspace: Design cities with appropriate greenspaces, including local and regional parks, green infrastructure, and out-of-city wilderness access programs. What this report makes clear is that improving mental health through urban design is not a nebulous aspiration: practical architecture and urban planning approaches that target specific risk factors are likely to yield results. Better population mental health is an essential contributor to a thriving, sustainable city, and this report contributes an important analysis that will be helpful to citymakers. Read the report
by Jenny Roe and Alice Roe Access to parks and urban green space facilitates exposure to nature, exercise and social opportunities that have positive impacts on both physical and mental health. In the last decade, rates of migration have risen dramatically across the globe: by 2038, it’s expected that half of London’s residents will be of a black and minority ethnic origin (BME). Our cities, towns and communities are becoming increasingly multicultural and, yet there are inequalities. A recent report by the Equalities and Human Rights Commission showed that in the UK, ethnic minorities are experiencing worse health outcomes. This is particularly the case for mental health: in 2012, the proportion of adults in England who were at risk of poor mental health was found to be higher among Pakistani/Bangladeshi and African/Caribbean/Black respondents than White respondents, and there were inequalities in accessing healthcare. Hence, it is increasingly important that research reflects the diverse make-up of these populations. A new study has sought to better understand the differences in use and perception of urban green space amongst BME groups in the UK, and illustrated the need for park facilitators to accommodate the needs, attitudes and interests of our multicultural population.  Source: Black Environment Network Several reviews have recently synthesised evidence showing the health benefits of contact with green space across a variety of international contexts but evidence of benefits by race/ethnicity is a notable gap. Given that BME groups in the UK generally suffer from poorer health and a wide range of environmental inequalities – perceiving their local open space to be poor in quality and reporting lower levels of use – the possible benefits of research into the relationships between green space, health and ethnicity is huge. While past studies have begun to identify different patterns of use and preference by ethnic minorities in urban green space, compared with white British populations, there is a need to better identify the underlying – and intrinsic – motivations behind these diverse behaviours. The study, conducted by Jenny Roe, Peter Aspinall and Catharine Ward Thompson, addresses this gap by exploring the role of urban green space in promoting general health within deprived urban communities in England. The study took an usual approach by exploring how aspects of social wellbeing – feelings of loneliness, perceptions of trust in the local neighbourhood, and place belonging – relate to general health, alongside the physical neighbourhood characteristics of deprived BME and white British communities, including perceptions and use of local green space. Using a self-rated general measure of health, the study explored individual, social and environmental predictors of general health in six ethnic groups living in three of England’s most ethnically mixed conurbations (i.e. London, Manchester and the Wolverhampton and Coventry area). The results of a household questionnaire, given to 523 people, identified three distinct health groups according to ethnicity: (1) people of Indian origin, who recorded the best health, (2) white British and (3) a segment labeled ‘Mixed BME’ combining people of African-Caribbean, Bangladeshi, and Pakistani origin, and ‘Other BME’ (e.g. people of Chinese origin and other white background), who reported the worst health. A key finding was that aspects of social wellbeing predicted general health in all three health groups. Trust was a high ranking predictor of general health, particularly amongst people of Indian origin, compared to our ‘Mixed BME’ group, where place belonging ranked more highly. All of our measures of social wellbeing were found to be highly correlated to perceptions and use of community green. Significantly, general health in the worst health group (i.e. those ethnicities within the ‘Mixed BME’ group) was far more likely to be predicted by variables in urban green space usage and perception than in any other health group. Those of African-Caribbean, Bangladeshi, and Pakistani origin, and Other BME, perceived the quality of local green space to be poorer (i.e. less safe, less attractive) and their visiting patterns varied significantly between winter and summer. In particular, low level of visits in winter was a significant determinant of poor general health. By comparison, the best health group (i.e. people of Indian origin) rated their neighbourhood more positively and felt greater levels of place-belonging than the other two health groups. For people of Indian origin, walking to a local urban green space was a predictor of good health, and they were much more likely to be accompanied by someone during visits (90%). The study identifies a clear correlation between self-reported general health and levels of use and perception of urban green space amongst BME communities and, consequently, points to a need for health policy to better understand how to foster positive use of urban green space amongst ethnic minorities throughout the year. By exploring the differences in use and perceptions of urban green space by ethnic group, the study identified the need for urban planners to take into account the diverse usage patterns of minority groups. For instance, we know that young women of Asian-British origin will be more likely to visit local green space if they can find a space to be among women of their own ethnicity. Park planners and recreational facilitators must therefore make a pronounced effort to understand these patterns of behaviour in order to better, and more appropriately, provide for BME groups. The study made clear the need for a culture of health specific to locality, race and ethnicity and the need for an intersectional approach to research – which is able to understand differences according to ethnicity, gender and poverty – to become the norm. About the Authors
Further information This op-ed is based on a new study by Jenny Roe and colleagues:
Roe J, Aspinall PA, Thompson CW. Understanding Relationships between Health, Ethnicity, Place and the Role of Urban Green Space in Deprived Urban Communities. Int. J. Environ. Res. Public Health 2016, 13(7), 681. doi:10.3390/ijerph13070681 |
Sanity and Urbanity:
|









 RSS Feed
RSS Feed