SANITY AND URBANITY BLOG
If you are an academic, urban designer, planner, health professional or citymaker, and would like to submit a blog, please see submission guidelines.

|
UD/MH Director Layla McCay made the intrepid trip from Tokyo to Okutama Forest to experience shinrin yoku, also known as forest bathing, a Japanese practice to improve mental and physical health. She wondered about lessons for urban design. Her experience could only be captured in the form of a comic interlude... Around a quarter of people in urban Tokyo are said to regularly participate in shinrin yoku, or ‘forest bathing’. This Japanese practice was made official by the Ministry of Agriculture, Forestry and Fisheries in 1982. It means spending leisurely time experiencing the forest with all five senses. The point is to walk slowly and mindfully, appreciating the sounds, sights, smells, feel and taste of the forest, far from the screens and chaos of city life. Substantial research has found associations between spending this time in the forest and improvements in physiological and psychological indicators of stress, mood hostility, fatigue, confusion and vitality, including reductions in heart rate and blood pressure. I love hiking and I usually find it serene. So how does shinrin yoku differ from the ordinary hiking experience? First, only a limited number of specific forests in Japan have been designated as official shinrin yoku sites. Designation requires a wide variety of criteria to be met, from ensuring visitors can experience the forest with all five senses, to having specifically tall trees, to scientifically recording health impact, to ensuring trained forest assistants are on hand. None of these assistants were in sight when I got off the train at the only official shinrin yoku site within Tokyo’s borders: Okutama Forest. But the woman in the visitors’ office kindly provided me with a hand drawn photocopy of the routes and marked one for me in pink highlighter pen. Then, with her vague point in the right direction, I was sent on my way. The other hikers who had been on my train inexplicably vanished and soon I was alone in the forest, ready to find out how shinrin yoku differs in practice from ordinary hiking in a forest. Without a proper guide, and being a little too much of an urbanite, I don’t know if I really found out. But since you didn’t get to join me, I will bring you inside the experience by welcoming you into my thought process over an hour and a half, one sunny Tuesday morning.
Walking down these steps, I see so many trees and greenery. I smell the forest. I hear the burbling river. It’s so serene. So quiet. I hope it’s safe that I came here alone. Oh my goodness, what’s that noise? Oh, it’s my paper map crinkling in my hand. So 1990s. How lovely to have escaped technology. Better look at the map. Hmmm the route is very unclear. Cross this bridge? Maybe not. Oops, I think this is the wrong direction. Reverse. Google Maps has destroyed my orienteering skills! Oh, but I do have my phone. Okay, let’s check Google Maps. Google Maps doesn’t have this route. Hmmm this is not very relaxing so far. Oh, but here’s a sign, and it's in English. I apparently just walked the Okutama Fureai Shinrin yoku course, Hikawa Ravine without even realizing. That wasn’t a very dramatic ravine. Or shinrin yoku experience. Onwards.
Oh, a paved road. That’s partly disappointing and partly reassuring. Also, a vending machine. Mmm cold lemonade. Delicious. Not sure that’s the taste of the forest the shinrin yoku experts had in mind. Hmmm the directions to the next route are written in Kanji. I’ll ask Google Translate. Urgh, Google Translate is bad at reading kanji carved into wooden direction posts. But I do recognize that one kanji means mountain. Think I’ll go the other way. That was the wrong way. Reverse. Ouch, these ferns are jagging into my leg. Aaargh a wasp! Or could it be one of these deadly Japanese hornets? Pep talk time. Come on, enjoy the nature. Oh okay, maybe this is the next forest bathing entrance. Japanese people clearly like to keep their signs subtle… No, that was someone’s garden. Oh okay, THIS is the entrance. Yes! Forest therapy. The Toke Trail. Now we’re talking! This is cool. The other therapy trail felt like just an ordinary hiking trail. This one is fancy. It has gravitas. It starts with a well kept, modern little hut. Oh, it’s locked. Hmmm maybe Tuesday morning is a sub-optimal time for forest bathing. Is the whole trail closed? No. Onwards!
How lovely that they have a special little train track and carriage for people in wheelchairs or who have other mobility challenges. Also, the walking trail is nicely kept, covered in chipped wood. The mountain views are beautiful. The trees are so tall. The sun is so bright. Hmmm, better stop and put on some sun lotion. Come on, be more mindful! Oh this is nice. Charmingly designed. Lots of little chairs and tables of different types, tastefully blend into the scenery, encouraging you to linger and appreciate the scenery. Little viewing stations where you can curl up in a nook and look directly out into the forest. Maybe I’ll do that later. Wonder what the long, sloped table is for. Probably should have come on a weekend – they probably have activities. It’s so secluded today. I’m the only person here. So lovely.
Oh gosh, it’s a snake. Okay, freeze. Assess.  Yup, it’s a snake. It’s quite long. About a metre long. And it’s turned to look at me. Why is there nobody else on this path? Is it a poisonous snake? How would I know? Google: Okutama forest snakes dangerous? Google result: 'The world’s deadliest snakes', '25 of the world’s most venomous snakes', '10 most poisonous and most dangerous snakes in the world'. I may have to stand here frozen forever. Facebook: 'Alone in the forest and too scared to walk past a snake. I knew hiking alone was a harebrained scheme. He’s looking at me. Help!' (photo attached) Facebook result: One like, three open-mouth emoji faces from urban friends. Twitter: 'Snake etiquette please? March past him and hope for the best? Turn around and abandon walk?' (photo attached) Twitter result: 'Doesn’t seem to be a viper which is good, so I’d walk past slowly, trying not to disturb him/her.' Duly chastened for making gender assumptions about snake. Close eyes and dash past, in direct contravention of the slow walk instruction. Snake does not pursue. Though I am convinced he/she does for about 100 metres. Heart pounding. Remember the research about the heart rate-reducing properties of the therapy walk. Alas. Walk more rapidly than appropriate for a therapy walk. See a twig. Scream preemptively in case it’s a snake. Why is there nobody else on this path? Pass hut number two. Locked again. Has yoga things inside. It would be nice to do yoga while looking out at the forest. But it’s not for me, apparently. Onwards. Aaargh a… twig. Okay. Stop this. Enjoy the nature. What’s that noise?! Oh, my map crinkling again. Aaaargh something’s on my face. Oh, a spider web. Not relaxed. Text friends to tell them I’m still alive. They are at work and unmoved. Hut three. Tell Twitter I’m still alive. Twitter asks if I have a bear bell. I do not, but suddenly recall the jangling of bells from fellow hikers on the train. And the picture of a bear outside the station accompanied by Japanese writing I failed to read. Apparently I now have to sing to protect myself from bears. Relaxation is further diminishing (along with that of any person within earshot – of which there still appears to be none). Thank goodness, a paved road. Oh, I mean Awwww, what a shame the therapy walk is over. Oh, a ten minute walk down the road and I can pick up the Fureai Shinrin Yoku path again. Aaaargh, what was that? A twig. I see three helicopters overhead. I wonder if Twitter has sent someone to rescue me. Another signpost, another Google Translate fail. But aha, do I see the character for station? I believe I do. I’d brought a picnic but am too paranoid to eat it til I’m back in town and there are no more scenic picnic tables. Well that was a bit embarrassing. I think I did shinrin yoku wrong… On the train back to the city. All the hikers’ bear bells are jingling as they serenely look at me, and they seem to be thinking: 'well, if you brought your laptop on shinrin yoku, you were already doing it wrong'. About the author
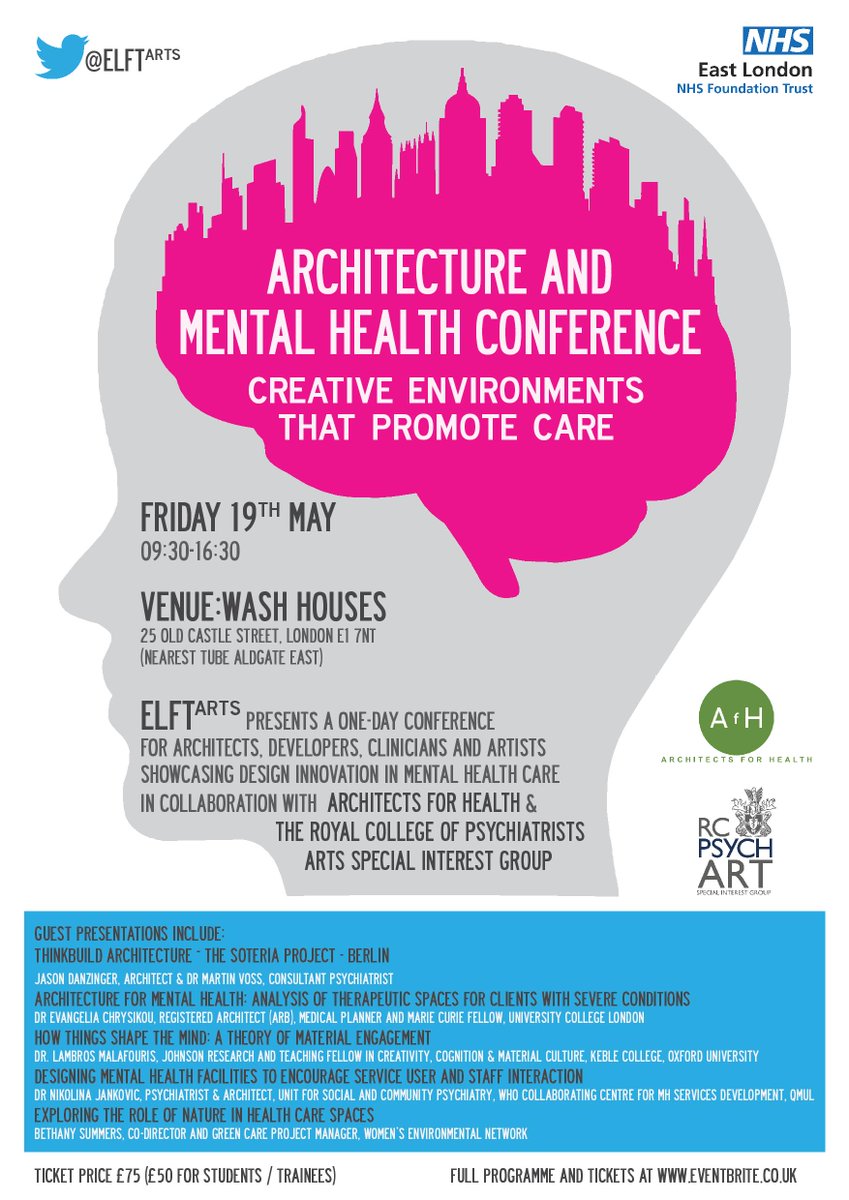
Jacob King of the London School of Hygiene and Tropical medicine and UD/MH Associate reports from the Architecture and Mental Health Conference jointly run by Architects for Health and the Royal College of Psychiatrists on 19th May 2017.
Components of design for mental health Physical characteristics of an environment that promotes good mental health The day was focused around the presentation of cases of innovative, evidence based designs stretching from corridors and bedrooms, to bridges, gardens and entire psychiatric hospitals within the community. From each of these designs evolved a few recurring themes. Notably, that certain physical characteristics of environment are favoured for mental health promotion: open spaces, bountiful light, quietness, greenery, and cleanliness. Social spaces were considered essential, and multiple speakers highlighted the importance of spaces which function communally, designed to increase conversation and group activity. Yet the opposite was also deemed important: there should also exist spaces which are personal, isolating and foster feelings of security, ownership, and separateness. Finally, the need for spaces which are able to facilitate fruitful occupation was repeatedly identified. As such, designers seek to achieve an appropriate and accessible mix of social and asocial environments between which people can choose according to will . The environment required of a psychiatric hospital is vastly different to that required of other settings. In particular, security must take top priority, there must be detailed environmental assessment for ligature points, and an understanding of which spaces are conducive for relaxation as much as being propagatory of violence and distress becomes key. While these priorities may pose a challenge to architects aiming to design a sense of freedom into their building, arguably this challenge should be tackled in much the same way as “designing mental health” into non-institutional settings. Bringing good design from the psychiatric hospital to the wider community Designing for mental health is often focused on the psychiatric hospital, and while this is important it is right that more emphasis is now being placed on non-institutional settings: the workplace, home and community milieu. Perhaps there is public health benefit to be realised from assessing the few core architectural features which promote mental health and studying how we can incorporate these, not only into psychiatric hospitals but into all architectural design projects. Simple design features like changing the colour of flooring or walls, the height of the space, and setting ‘boundary markers’, can establish psychological zones: demarcating personal quiet spaces from communal social spaces. Innovative ‘greening’ methods may introduce nature inside, or better yet, creative use of lighting, windows and exploiting pretty surrounding views can metaphorically do the same job. Access to gardens or an orchard (as in Bethlem Royal Hospital) and the ability to wander and observe the changes in the seasons may have some effect in breaking one from the monotony of a sterile interior, providing another route towards emotional and psychological comfort. Leveraging architecture for behaviour change for mental wellbeing In acknowledging that architecture can fulfill the functional needs expected of it (a psychiatric hospital being secure, a place of business being productive, a residential space being cosy etc.), we accept that certain behaviours can be architecturally promoted or deterred. At this conference several projects were presented showcasing attempts to change individual behaviour for public mental health benefit. The first among these took on the task of structural environmental intervention for suicide prevention. Preventing suicides at the Derry Foyle bridge. The prevention of jumping from buildings and bridges has been a focus of discussion across the globe. Infamously one Chinese factory insensitively installed netting around the outside of its building to catch its workers who would jump. In Northern Ireland, the Foyle bridge in Derry/Londonderry is known widely as a local 'suicide hotspot'. A folk narrative has developed around the bridge, drawing people from across the surrounding areas to this spot, as Beachy Head does in England, to kill oneself in a ‘traditional’ way. The Our Future Foyle programme, funded by the Royal College of Art among other partners, aims to break this narrative and prevent suicides from the Foyle bridge. With multiple facets, the first step of this programme will revitalise the area surrounding the bridge with community events and business opportunities. Individuals attempting suicide often prefer to do so alone and out of sight of others. Therefore, by increasing footfall in the area through commercialising and pedestrianising the river bank and improving transport links, it is hoped that people will be dissuaded from jumping from the bridge.  The Foyle bridge: the view from the Derry city side. Photo credit: Wikimedia Commons. The next step concerned the role of suicide barriers on bridges. Often these barriers themselves are devoid of artistic thought and become an extension of the suicidal narrative of a building or bridge: “Those barriers are there to stop people jumping off”. This project aims to install functional art, a series of connected five metre tall metal reeds, to echo the reeds on the river bank below. While acting functionally as a suicide barrier, the reeds will also feature multi-coloured lights at their peaks, which can be changed by those promenading past, creating new narratives associated with this place. This idea of urban design is striking, especially if it is eventually proven effective in preventing suicides. By changing the narrative of a space, its social typology, and incorporating functional architecture - both social and physical barriers to suicide attempts - we wait to see if there is an effect on the prevention of suicide, a major mental health outcome. New models of asylum Asylum in the heart of London The location of psychiatric hospitals is an important facet of urban design, making bold statements about society’s relationship with psychiatric patients. Historically this has been a point of contention. In London for example, as the city expanded outwards, asylums which had previously been on the outskirts of the city were pushed further and further back into the surrounding countryside. While the ethos of 19th century moral therapy also often included natural retreat, the “Not In My Back Yard” stance of many of London’s population unquestionably contributed to the construction of newer asylums in the surrounding countryside. Yet this trend is now evolving, and an example is the imminent revitalisation of the Springfield University hospital, an old asylum built within large grounds in South West London. The grounds will be turned into new community homes, with a new psychiatric hospital at its heart. Wards will be built above shops. According to the architects' drawings, there will be a view from inside these rooms of happy attractive people bustling around a communal square, shopping, and enjoying the sun. What may at first appear to be an attempt to commercialise prime real estate in London may turn out to play a key part in destigmatising psychiatry and rehabilitating patients to community living much more readily than an isolated and unintegrated asylum of old. MadLove: a designer asylum Following their success as an exhibit at The Wellcome Gallery earlier this year, MadLove: a designer asylum is a service user-led art movement aiming to collectively design the “most crazy, bonkers, mental asylum we dare dream of”. A space which is both safe and nurturing of madness the lead artists, both service users themselves, suggest that psychiatric hospitals can often be more punishment than love. After multiple rounds of consultation a collaborative plan was developed and showcased.  MadLove: a designer asylum. Photocredit: MadLove, The WellcomeTrust, November 2016. The MadLove design features tree-house style accommodation on a grassy hill, and a central hub with shops and occupational space. Someone is always available here to talk or relax with. The sounds of birds and the sea breeze (which carries in the smell of baking bread) can be heard around the asylum. There are no fences and residents come and go as and when they please. The results of their extensive service user consultations are freely available online. Conclusion: evidence based design + participatory design = mental health Architecture is just one tool of the urban planner, but it is essential in propagating mental health benefit to a city’s residents. In closing the conference, one architect made a plea to the audience - seconded by service users and psychiatrists alike - that design should be first, evidenced based, and more importantly built in collaboration with those who will live and work in their buildings and environments. The need for both evidenced based design and participatory design strikes at the heart of how architecture can foster effective mental health-promoting features of design, and reduce the often emotional and physical imposition of a building's primary function: security, sanctuary, or productivity alike. About the author
by Layla McCay, UD/MH Director UD/MH is often asked about how mental health principles can be applied in different conflict and post-conflict situations. This week in the medical journal The Lancet, a review was published on the public health impact of 'explosive remnants of war'. The researchers highlight that beyond the physical injuries landmines and exploded or unexploded ordinance can cause to displaced people returning home after conflict, they also seem to exert significant impact on people's mental health. This can include anxiety, depression, and post-traumatic stress disorder (though a direct causative link could not be made). These mental health effects can occur even where the explosives are present but have not caused injury.
The paper does not speculate at length upon the reasons that these explosives may be linked to mental health problems. I wonder if an important contribution is how they can affect the meaning of a place. The concept of ‘home’ is important for people’s sense of belonging, and as such, affects their mental health and wellbeing. Place is the canvas onto which people project their personal and shared memories and expectations. A place feels like ‘home’ because it brims with personal landmarks (the café at which we spent hours laughing with friends, the first apartment we lived in, the park bench from which our child leapt, playing astronaut). For many, home is, by definition, a safe place (or at least there are places where we know we can go to feel safe). Yet when people return home after conflict, they sometimes find that conflict has changed the meaning of the place that was once home. It is difficult to recognise. Personal landmarks become superimposed with physical and memory landmarks of fear and pain and sorrow and unease and trauma. When people lose the ability to reliably differentiate between safe and threatening, their perception of home evolves into a traumascape of disconnection and distrust. Urban design has an important role to play in helping the feeling of a place revert to 'home' after conflict. This means healing without forgetting: reducing the physical scars of conflict, and designing a place that engenders confidence and pride, that supports mental health and wellbeing, such as reliable infrastructure, green spaces, social spaces, places to walk and exercise, and places to feel safe. Engaging residents in designing the right approach to rebuilding can have benefits in also rebuilding the community: strengthening social capital and trust, while empowering people to take control of a place and help bring back the meaning of the place as a home they recognise. Explosive remnants of war, such as landmines, can confound these efforts, because a place can never feel entirely safe. War is still just beyond the doorstep. In avoiding and fearing the open spaces where people might otherwise have exercised, socialised, relaxed, and enjoyed nature, the prospect of finding home may be held in a state of suspended animation. People cannot trust their home not to harm them, and so they wait, walled in and tense. The Lancet paper reports that international support for mine action is declining. And yet it is an essential part of rebuilding - not just physical rebuilding, but a rebuilding a community's trust that they are home. For more on this topic, read UD/MH Fellow Sophie Gleizes on traumascapes. Jacob King and Jianan Bao, London School of Hygiene and Tropical Medicine reflect on the Global Ageing: Challenges and opportunities conference hosted by The Royal Society of Medicine in London UK on 24th and 25th April 2017 on how future demographic and geographical changes will affect the health of increasingly older populations. If it was not already abundantly clear that we are hurtling directly towards the Age of the City, this conference made the point inescapable. City living permeates health through and through. Not only the root of psychosocial, cultural, economic, biological risk factors and protective health factors alike, The City fundamentally shapes the way we interact with health care too. Concurrent with universal mass migration into cities, global aging and super-aging offers substantial new challenges to health. The global population is ageing exponentially Opening the conference with a detailed review of the future demographic and geographic changes affecting our shared home was WHO director of the Department of Ageing and Lifecourse, Dr John Beard. Published in 2007 the WHOs “Global age-friendly cities: a guide” framework will be familiar to many readers. From this starting point Dr Beard highlighted the substantial demographic changes in age across developing areas of the world. He explained that while developed countries like the UK saw national life expectancy slowly grow from 40 to 60 years between 1800 and 1920, India saw the same age jump in just 35 years (1960 - 1995), and China in just 15 years (1950 - 1965).(1) Populations largely naive to supporting large numbers of elderly citizens are similarly those most faced by the challenges of rapid urbanisation. World Urbanisation Prospects, from the UN highlights that while currently around 54% of the world’s population live in cities, by 2050 it will have increased to 66%, with 90% of this change coming from Africa and Asia.(2)  Major new housing construction project in Zheijiang, China. Photograph by Jianan Bao The rise of dementia Importantly, old age represents a rather different profile of mental health conditions compared to other age groups. Old-age psychiatry stands as a separate area of subspecialty within psychiatry for exactly this reason. While mental health problems affect people of all ages (for example, older people have similar rates of depression to other age groups (3), dementia stands almost uniquely as a mental health condition that predominantly affects the elderly. Dementia is set to increase rapidly around the world, especially amongst people who live in low and middle income countries as a consequence of longer life expectancies and changing risk factors for disease. Given a standardised age profile, dementia affects 5-7% of the population, a rate that is constant across all countries. Dementia causes more disability than any other condition in elderly people and with that comes the need for care, a need which puts a great strain on countries without the infrastructure for domiciliary care. Unfortunately this often results in huge economic losses for households that may need to provide sometimes quite intensive care for relatives with dementia. Carers of people with dementia may find it difficult to travel long distances for care, resulting lower rates of healthcare utilisation in this group of people for whom social and health care needs are high, and more often than not unmet.  A group of Hangzhou residents doing their morning exercises, 2008. Photograph by Jianan Bao Assessing the cognitive footprint in urban design Dementia is only the tip of the iceberg; cognition and cognitive impairment lies underneath the surface, and to tackle that could reduce the rates of dementia. Many factors similarly contribute to cognitive impairment: exercise, pollution, loneliness, poverty. Professor Martin Prince pointed out that a reduction of risk factors by 10% could reduce the prevalence of dementia by 8%. There is a clear opportunity therefore to address some of the risk factors of city living which are also implicated in cognitive decline through thoughtful urban design. Professor Rossor suggests that concept of a ‘cognitive footprint’ should be considered when assessing the impact of policies: how will this affect cognition and brain health? There is good evidence that some factors associated with city living are good for mental health: higher employment, better healthcare access, varied recreational opportunities. However, many negatives co-occur: fewer spontaneous opportunities for exercise, less societal integration, fewer green spaces, safety fears, and noise and light pollution. (4) Physical limitations, cognitive decline, a different profile of mental and physical conditions and perhaps relative lack of social support among older people make the mental health implications of cities different to other groups. Yet, overall, only patchy evidence applies the bio-psycho-social variations in the elderly experience of city living to mental health outcomes. Despite the increase in funding for dementia, as a field of research it suffers from a lack of researchers. At the conference, Professor Rossor called for more interdisciplinary research in this field involving biomedical researchers, sociologists and of course urban planners. Healthy cities in a global context Over many years numerous associations between the urban environment and mental health have been established. Elderly residents are more likely to spend time in the area surrounding their homes than younger adults who commute away for work. Prof Anthea Tinker in her workshop “Age-friendly cities in a global context” outlined the effects of neighbourhood qualities on numerous health measures. The so-called “walkability” of a neighbourhood is directly related to the amount of exercise elderly populations take. Furthermore this relationship may have benefit to mental health too. Evidence suggests that environments which are distinctive, recognisable, familiar are often reported by people with dementia as more comforting. Changes in urban design which therefore make a space more accessible: safe, walkable, but remain familiar are therefore likely to promote its use and quite possibly more than just mental health benefit. Green Space A particularly important opportunity for urban design is green space. Professor Caroline Ward Thompson, Professor of Landscape Architecture at University of Edinburgh discussed how green space exposure impacts the mood of older people. It is clear from observational studies over many years that exposure to green spaces is good for mental health. But does it exert more or less impact for elderly people? How does physical decline affect this population’s ability to access green spaces? In her work Prof Ward-Thompson employed neuroimaging techniques, notably EEG (electroencephalography) to assess the experience of stress in green environments. In short, there seems to be evidence for the relaxing effect of walking in green space. To these writers’ relief, there was a strong feeling in the room that any practical applications of this knowledge should be reified through protecting and increasing the availability of green spaces and making them more accessible to the elderly. There is a danger that because of the difficulties of elderly populations accessing parks and especially so fields or forests, that artificially creating mock up green environments in elderly people's homes is an easy alternative. The “active ingredients” of green space exposure on mental health and mood are still largely unknown. Further studies to assess what exactly delivers the benefit - the exercise, the quiet or light, the greenery itself for example - are needed.  Photograph: Håkan Dahlström - Green picnic, CC BY 2.0, through Wikimedia Commons. An emerging design challenge: facilitating older people's participation in the workforce Recent work by speakers Dr Mauricio Avendano and Professor Karen Glaser examined the complex associations between mental health and retirement. They noted that some retirees giving up work receive a boost to their mental health, particularly when the retirement is planned but many others do not, particularly those who are forced to take retirement due to physical and/or mental health problems. (5) Given the health benefits of employment, alongside the economic unfeasibility of ever-longer periods of retirement, they proposed that retirement age should rise in line with aging populations. In this light we may have to find ways to facilitate longer working lives, and better incorporate different physical and cognitive abilities in the workplace. For urban designers, this sociological shift could mean examining the concepts of elderly commuting, and creating different sorts of work environments.  Elderly tourists near West Lake, Hangzhou. Sign reads: no vehicles allowed. Photograph by Jianan Bao War, displacement and the elderly Anthropologist Dr Hannah Kienzler and clinical academic Prof Richard Sullivan discussed the implications of war upon elderly populations. We frequently hear on the news about conflict zones around the world, but little time is spent considering the burden on older adults. The elderly population tend to stay within regions of conflict, in part due to the high risk associated with fleeing with potential sensory disabilities and health conditions (and indeed refugee camps often have challenges providing long term care). Dr Kienzler identified the role of older people as carriers of knowledge with a key role to be harnessed in post-conflict community rebuilding and humanitarian planning.  Posters A number of posters were presented on the day, including one by UD/MH associate Jacob King titled: “Urban environments and depression in older adults: Designing mental health promotion into our cities” Concerning similar themes to Prof Tinker’s workshop, in the poster he suggested that mental health promotion can be built into cities. We have already seen that there may be benefit in making use of green space more accessible, making a neighbourhood more walkable, and community facilities more accessible, and so on. In short by following public health concepts originally developed in the fight against HIV, an intervention, an urban design feature, should be available, accessible, and acceptable. (6) For example, walking around a neighbourhood may be acceptable if it is safe, perhaps with fewer cars or less busy pavements. A green space could be accessible if there were well maintained flat walks ways and situated within a reasonable distance to residences, or indeed incorporated into one’s routine environment. And most simply, health care services are only effective if they are available in an area. 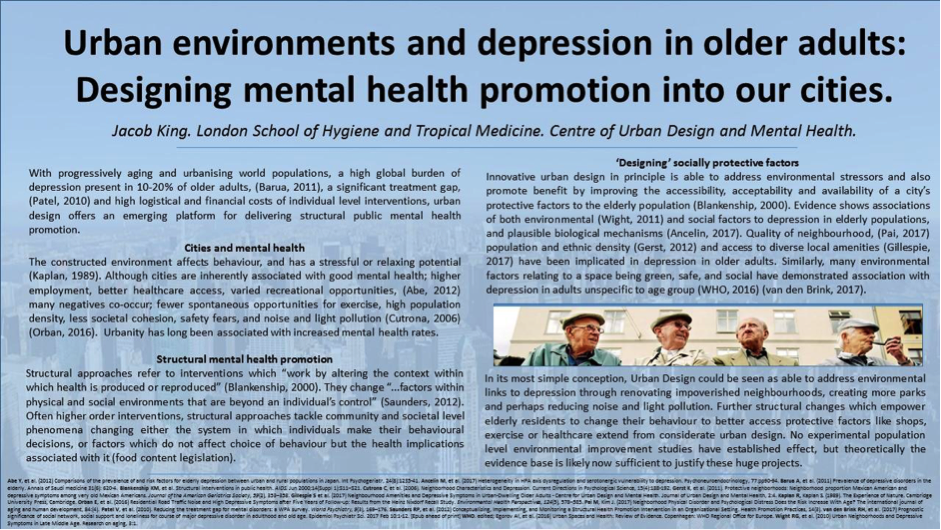 Concluding remarks Only a limited number of factors which constitute the vast number of associations of city living, older adults and mental health could possibly have been explored at The Global Aging Conference. Several key facets, access to local amenities and health care, and social care and loneliness were notably missing. But while nothing especially new or ground breaking in the field of urban design and mental health was established at the conference, we reasonably believe that such emphasis, as was placed by 3 workshops and a selection of poster presentations, marks a notable step for a high profile medical conference. Employment, green space, neighbourhood quality are indeed three highly important areas in the urban space mental health connection. While rigorous evidence for the association of these factors is still in its early stages, each offers an interesting reference point to begin thinking about how the specific needs the elderly population require of their urban environment for good mental health. References
About the Authors
By Sus Sola Corazon, Assistant Professor at the University of Copenhagen, Department of Geosciences and Natural Resource Management. At present, studies on health-promoting environments are dominated by research focusing on the difference between the urban and the natural environment and less is known about which qualities of the natural environment promote mental health. Aim of the research Therefore the research group Nature, Health & Design at the University of Copenhagen, initiated a qualitative research project in the Danish Health Forest Garden Octovia. The aim of the project was to gain knowledge of which qualities and features of the environment were perceived as restorative. Methods The design of the Health Forest Octovia, where the research took place, is based on Grahn & Stigsdotter's research on perceived sensory dimensions (PSD). The Health Forest is located within an existing Arboretum and consists of eight different spatial settings. 26 female students participated in the study. They were individually interviewed about their restorative experience while participating in a guided walk through the health forest. Key findings that are relevant for planners and designers
Read the full research paper for free for further details Citation: Ulrika Karlsson Stigsdotter, Sus Sola Corazon, Ulrik Sidenius, Anne Dahl Refshauge, Patrik Grahn. Forest design for mental health promotion—Using perceived sensory dimensions to elicit restorative responses, Landscape and Urban Planning, Volume 160, April 2017, Pages 1-15 About the author of this blog
By Erin Sharp Newton, Assoc. AIA, M. Arch. Winter is on the wing, and spring is filtering in with fresh air, fresh thought and sunshine... and Mental Health Awareness Month. This annual opportunity to raise public awareness about mental health was established by the National Association for Mental Health (now Mental Health America) in 1949, around the same time as legislators were founding the Housing Act of 1949, which would instigate urban development and renewal in America, and thus start to reshape our cities. Although the Housing Act plans did not pan out as originally intended, what was begun was a serious start to looking at how cities and the built environment could be inclusive and supportive of all citizens. Of interest is what happens when we combine Mental Health Awareness with the built environment. How are we as designers, planners and citizens integrating what the past 68 years have shown us to do, or as Jane Jacobs would say, what to not do?
Each year a theme is presented for Mental Health Awareness Month, which is explored through the rest of the year. This year’s theme is “Risky Business” and focuses on the diverse risk factors for developing mental illness. The upcoming Mental Health America Annual Conference is aptly titled Sex, Drugs, and Rock & Roll, and will examine some of these risk factors.  “We believe it's important to educate people about habits and behaviors that increase the risk of developing or exacerbating mental illnesses, or could be signs of mental health problems themselves. These include risk factors such as risky sex, prescription drug misuse, internet addiction, excessive spending, marijuana use, and troublesome exercise patterns." - Mental Health America (MHA) However, risks to mental health are not confined to individual factors. The built environment can help create and maintain risk factors for mental illness by increasing stimulation while stripping away protective factors for good mental health, for example:
Architects, urban planners and designers can make an impact. We, as designers of the world around us, can Mind the GAPS to help address these risks. We can open doors, create opportunities in our cities, societies, and communities to support awareness and address risks to improve mental health for all. We can dive into our own creative intelligence and promote green space, walkable cities, and infrastructure that allows us to move around and express happiness & health. We can look for where our efforts support or create opportunities for social interaction, community support, and personal freedom. We can advocate for creative space, for communal space, and for safe, meditative place. Through these efforts we can play a role in improving mental health across the board. Designing healthcare facilities, buildings, public spaces, and communities that take into consideration all the sensitive aspects of being unwell, creating humane opportunities for refuge (or outlet), and pro-actively advocating the development of physical places for healing and wellness. Being knowledgeable about what hurts, what helps, what heals. These are starters. We can:
 Jay Pritzker Pavilion, Millenium Park, Chicago (Illinois), USA, Wikimedia Commons “Under the seeming disorder of the old city, wherever the old city is working successfully, is a marvelous order for maintaining the safety of the streets and the freedom of the city. It is a complex order. Its essence is intricacy of sidewalk use, bringing with it a constant succession of eyes. This order is all composed of movement and change, and although it is life, not art, we may fancifully call it the art form of the city and liken it to the dance — not to a simple-minded precision dance with everyone kicking up at the same time, twirling in unison and bowing off en masse, but to an intricate ballet in which the individual dancers and ensembles all have distinctive parts which miraculously reinforce each other and compose an orderly whole. The ballet of the good city sidewalk never repeats itself from place to place, and in any once place is always replete with new improvisations.” ― Jane Jacobs, The Death and Life of Great American Cities Although it can be challenging to think about mental, emotional, and behavioral health problems, ignoring them won’t make them go away. When there is illness, it affects those nearby. When many are ill (as in 1 in 4 estimated) it affects society at large. It is necessary to take good inventory of the risk factors within the built environment, if we are to help rebuild, strengthen, repair and recover. Further information Urban design and mental health:
Mental Health Awareness Month:
About the Author
|
Sanity and Urbanity:
|














 RSS Feed
RSS Feed