SANITY AND URBANITY BLOG
If you are an academic, urban designer, planner, health professional or citymaker, and would like to submit a blog, please see submission guidelines.

|
by Matthew Williams PhD Independent Researcher / Sustainable Urban Mobility Consultant, IIGH-UNU Does the way we move around our cities make us, and the planet, healthier or indeed happier? In order to answer this question, we need to take a step back to understand why we move around our cities as we do today. In the twentieth century, car companies, urban planners, and national governments focused more on GDP than well-being, sold us private transport. Car corporations, backed by national governments, built lots of cars, planners laid out sprawling cities to accommodate them, city officials invested more in road infrastructure than public transit, and advertisers told us we needed a car to be happy and show our peers we were successful. In many cities, such as Atlanta and Kuala Lumpur, people have been left with no alternative but to buy a car, unless they cannot afford one. Then getting around the city can be very problematic. The result in many cities is private automobile-dominated transport systems, with entrenched transport inequality. In other words, while the ‘haves’ drive cars, low-income groups take the bus. These groups also have diminished access to workplaces and social gatherings with friends and community groups when public transit is infrequent or of poor quality in cities built for cars. The Brazilian politician and urban planner, Jamie Lerner, writing in the New York Times in December 2015, points out that cars take up more space than humans, and the average 50 square metres of space that a car occupies when parked at home and at work, is equal to the size of a family home or workplace in many countries. What if, as Lerner asks, this space was available instead for small businesses? Instead of ‘each to his own’ in their private car bubble, we could replace the social isolation of car-dependent neighborhoods with the heightened sense of community found in more coffee houses, bookshops, pocket parks and walkable streets. By 2030 the number of cars on the world’s roads is anticipated to double to 2 billion. Much of that demand is coming from the burgeoning middle classes of China and India as they embrace the advertiser’s promise of ‘freedom’ and status on the open road, an illusion which slowly unravels with each traffic jam. However, a century of the car has revealed that such car dependence has known health and well-being impacts, falling into 5 areas: 1) road deaths and injuries, an annual average of 1.2 million deaths globally, according to a 2015 WHO road safety report 2) respiratory illness, cardiovascular disease and cancer associated with air pollution 3) obesity, diabetes and cardiovascular disease related to physical inactivity 4) social isolation and higher rates of depression in car-dependent neighborhoods 5) social and health inequalities, a sense of social exclusion of non-car owners, who nevertheless must breathe the pollutants emitted by cars. But the health of people and the environment are inseparable. The transport sector is the greatest contributor to greenhouse gas emissions which cause global warming. Climate change is leading to more extreme heat events, the effects of which are more intense in cities because of the urban ‘heat island’ phenomenon. The urban poor also suffer more from water-and-food-borne gastrointestinal infections, and vector-borne (e.g., dengue fever) diseases due to climate change. So, the way we move around our cities can make us sick, or even kill us in other ‘distant’ ways, not just on the road. The best hope may be to stop driving cars which burn fossil fuels, and use active transport such as walking and cycling, as well as mass transit.  Different people sharing a train carriage in Tokyo; photo by author However, we should acknowledge that cars do afford certain freedoms. They allow us to look after family members, for example, by transporting children and elderly parents to medical treatment, give us access to social networks and education and employment, and satisfy the consumer desires of some. However, the collective cost to society has been too high. As Jamie Lerner also said, ‘Cars are the cigarettes of the future’. So, no, cars have made neither us, nor the planet, healthier. And while individuals may experience a brief spike in happiness as with any consumer purchase, and derive happiness from looking after family members with cars when necessary, cars are not an enduring source of personal happiness. Collectively, the impact of many cars, their infrastructure (roads, parking space, gas stations), noise and emissions, degrades neighbourhoods and diminishes our happiness and well-being. We have now awakened to the fact that our cities have been designed primarily to move cars, rather than people. And, as the preeminent urbanist Jan Gehl poignantly reminds us, a city can be designed for cars or designed for people, but not for both. While the automobile has a place in the mobility mix, active transport such as walking and cycling and mass transit options such as light rail and Bus Rapid Transit are more desirable for a number of reasons. Firstly, they are designed for everyone, not only for people with the means to afford a car. They promote individual health by making us more physically active and reduce pollution-related illness. Less carbon-emitting cars on the roads means less greenhouse gas emissions. And when cities are designed for people, rather than cars, public space is reconfigured towards more walkable neighborhoods, which encourage social interaction and build social cohesion within communities. And as the famous twentieth century urbanist Jane Jacobs wrote in the 1960s, more walkable neighborhoods means ‘more eyes on the street’, the best and most natural form of security. When most people rely on public transit, namely middle class and low-income groups, social equality is strengthened, and non-car owners suffer less from the fumes of cars they cannot afford. Children can walk and cycle without fear of being hit by cars, the elderly are more inclined to venture outdoors, and green space is restored to spaces previously occupied by cars. And our sensory landscape becomes more attractive, when the sound of cars and the smell of their fumes give way to the underlying sounds of the city itself, and the smell of fresh air. Its is clear then that active transport , combined with public transit, makes us and the planet healthier, and makes for happier, more connected communities. Re-imagining mobility from a people-centred prism has had great results. In Mexico City, for example, new bike share systems are proving popular with women especially, a group that is often more vulnerable to transport exclusion, mostly due to safety fears. In Copenhagen, the preferred mode of transport for almost half of the population is the bicycle, and as the city ‘s Green Wave initiative is rolled out to make Copenhagen the world’s first carbon neutral capital by 2025, wireless LED lighting embedded in bicycle paths uses sensors feeding into software to provide information to cyclists about traffic conditions ahead. But as we embrace this technology, we must not lose the lesson of the twentieth century – that mobility should be designed first and foremost for people, whose happiness and well-being is found in the social ties of strong walkable, human-scaled communities free of car fumes and the threat of traffic injury. About the author
by Giulia Melis SiTI, Politecnico di Torino, Italy Since ancient times, we have known that the place where we live can impact our health. Cities have always been shaped and restructured according to the needs and priorities of the time. The Roman Empire, for instance, created a model for the planned city: with its rigid morphologic and geometric rules, the typical Roman settlement provided basic facilities and infrastructure for its inhabitants, ranging from thermal baths, to aqueducts and sewers. During the Industrial Revolution, cities had to face a new challenge: overcrowding, industrial dumps, and bad hygiene conditions were helping the spread of infectious diseases, and working class suburbs were growing too fast, without any concern about the quality of life in those areas. That’s how laws about urban décor, cleanliness and sanitation started to be discussed: the Public Health Act (UK, 1948) is one of the first examples. This Act linked the urban design of a city with the spreading of epidemic diseases, and tried to prevent it by moving industrial production out of the city core. This model lasted until recent decades, when deindustrialization and various crises meant the need for new paradigms. Nowadays, modern cities are starting to wonder not only how to create a healthy environment to protect the spread of epidemics, diseases, violence etc., but also how to enhance the quality of life of their citizens and their wellbeing. The waves of New Urbanism are questioning our lifestyles, and starting to re-consider the social component of city life as fundamental for granting us happiness and fulfilment. That’s why, as a group of researchers coming from the architectural and medical domain, we became interested in mental health in our cities. As urban planners, we were interested in understanding which urban features most significantly affect our daily life, in order to identify the most urgent and promising intervention opportunities towards less-stressful urban living. And as public health experts, we wanted to know if the effects are equally distributed among the population, or whether some groups are experiencing a higher burden? The Research We chose an Italian city, Torino, where a huge dataset on population health is available, and looked to see if the numbers confirmed our initial theory. While a lot of researchers have already presented evidence of the importance of urban trees and parks, which can have a profoundly beneficial impact on psychological wellbeing and general mental health, not many studies have analysed the urban built environment in its complex functioning. We therefore gathered data both on the structure of the city (how dense it is, where are the parks for recreational activities, which is the mix of functions in one area) and its services (is the nearest library placed within an accessible distance? is the area well-served by public transport? Are there public sport facilities? Cinemas, theatres? etc) and we looked for connections between this data and the consumption of antidepressant drugs in the city. 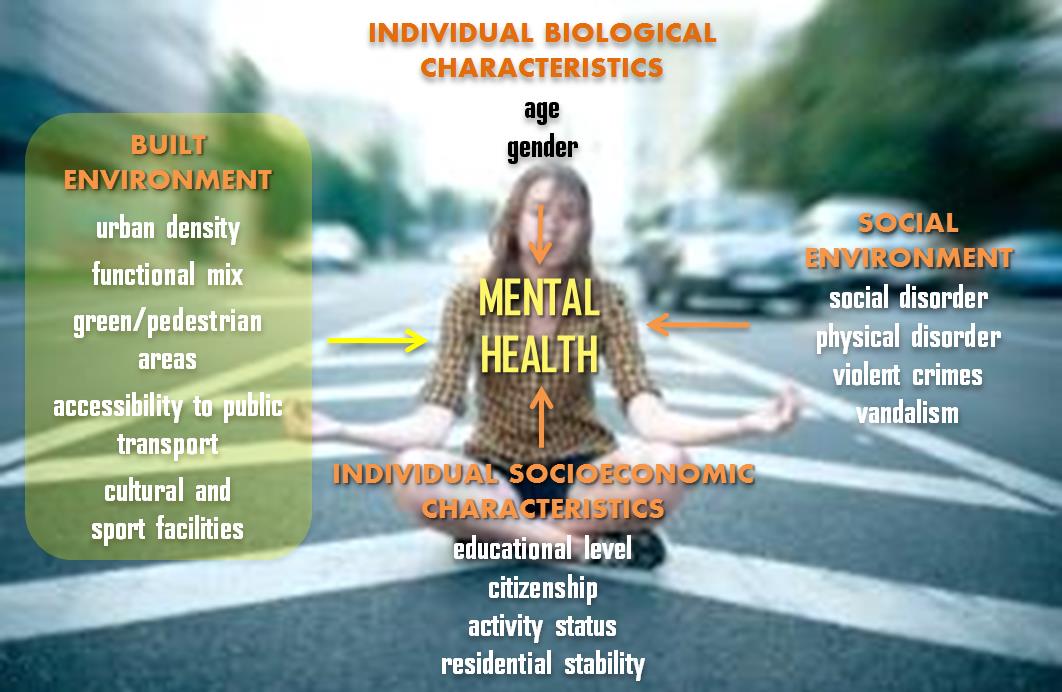 This scheme illustrates the variables considered in the study as plausibly connected to mental health in urban areas. The Results Our research suggests that good accessibility to public transport, as well as a dense urban structure (versus sprawl), could contribute to a reduced risk of depression, especially for women and elderly, by increasing opportunities to move around and enjoy an active social life. Women (of all ages) and older people (age 50 to 64) were found to be prescribed fewer antidepressant drugs when they lived in places reached more quickly by bus or train, and in places with taller average building heights, compared with counterparts in more remote or sparse areas. That connection held up even when social factors were taken into account. This means that if everybody had the same level of education, same citizenship, and were all in employment, all living in a neighbourhood that had equivalent levels of crimes and social and physical disorder, there would still be differences in antidepressant consumption according to how well the area is served by public transport and to the density and liveliness of the neighbourhood. Challenges and decisions with the method Antidepressant consumption is quite a strong indicator in mental health. Taking antidepressants implies that you have recognised you have a problem, actively sought help from a doctor, received a diagnosis and a prescription for antidepressant medication, and started treatment. This is a long way from starting to feel that you may be stressed or depressed. We used this indicator in our research as we were looking for solid evidence, but by doing so, it is likely that our results underestimate the phenomenon of stress and depression in the city, thus setting the stage for further and more accurate investigations and reflections. Of course the range of density that we were able to test was limited to that of a typical European city; this range does not include the extremes of US cities sprawl and high density (which are both known to have negative effects on health). Also, this type of large-scale data analysis can’t pinpoint causal mechanisms. But it’s not hard to speculate why transit and density might reduce stress: the former relieves the need to drive everywhere (and to own a car); the latter enhances the potential for social connectivity. For older populations, in particular, both aspects help guard against feelings of isolation or loneliness. They also stand in contrast to remote suburban living that “can have a serious impact on mental health, particularly when it results in forgone trips”.  The Conclusion There’s still a lot to understand about the key stressors of city life, but sound advice to urban planners could already be launched: in order to address health inequalities, urban policies should invest in the delivery of services that enhance resilience factors, above all a good public transport network, in a careful and equal manner, throughout the city. The Author
by Tracy A Marciano Urban Planning as a means to organize people, places, concepts and practices has an interesting history. As civilization progressed, urban planning followed a parallel trajectory, reacting to practices that outlived their usefulness. With each era, large scale redesign was at the forefront of change with small pockets of improvement on the periphery. Contemporary discourse about urban health is primarily focused on green spaces and walkability. While both are important in the urban fabric, they are not absolute measures of ideal public health and their results are hard to quantify against the variations in symptoms and treatments for mental disorders. Introducing concepts from other fields and recalibrating them into plausible urban design initiatives is a potentially interesting approach to improve mental health in cities. In particular, as urban areas gain momentum, exploring concepts from eastern medicine such as acupuncture, aromatherapy (or horticulture therapy), directional alignment with the sun and the moon, nocturnal gardens, botanical soundscapes and energy balancing might be applied to exert a positive impact on mental health in modern cities. 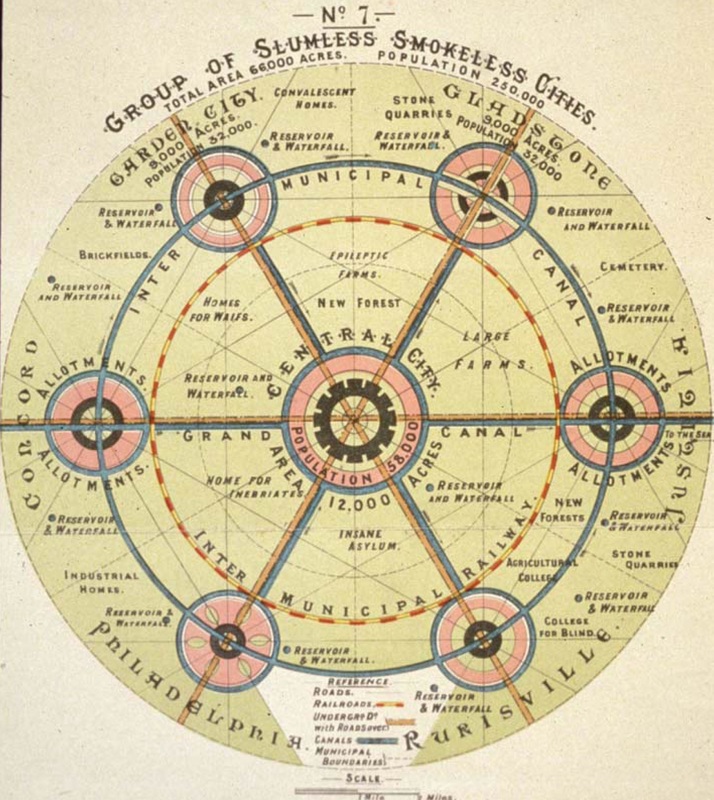 Map developed by Sir Ebenezer Howard, urban planner, 1850 - 1928. This shows his vision for improving the conditions of the poor through combining the best aspects of town and country and allocating space carefully. Read more here. As populations migrate towards urban centers at an accelerated rate, advancing improved health strategies - rather than utopia - is often being achieved through incremental improvements. A recent movement is New Urbanism, or tactile urbanism, which seeks to align with sustainability, preservation of existing buildings and walkability. However, as with past attempts at planning perfect cities, such as The Garden City movement, individual experience, public mental health and most importantly, the causation and impact of mental health problems have been largely excluded from the dialog. Jamie Lerner, who served three terms as the mayor of Curitiba, Brazil uses urban acupuncture as the philosophy behind his successful initiatives. Urban acupuncture is the mature cousin to tactical urbanism, which has suffered a bit of backlash lately as a trendy, high-concept practice of questionable long-term impact. Lerner writes in his book “Industrious mediocrity is gaining ground, along with merchants of complexity: the bean-counters and the inconclusive, never-ending researchers. But sometimes, just one stroke of creativity is acupuncture powerful enough to make progress.” In 2007 University of Minnesota published a paper about their collaboration with Blue Cross and Blue Shield of Minnesota. This paper highlighted key findings about how to increase accessibility to nature to address mental health problems. Their research also found that social networks are important and that mental health is connected to fundamental public health issues but did not offer developed solutions with measurable results. In most cities, areas that create tension and erratic energy and areas that can exacerbate anxiety, depression and isolation are evident. If cities are viewed as a biological system and receptive to holistic wellness plans, the philosophy of urban acupuncture may be an ideal platform to improve heath. For example, if obstructed walkways and clogged streets create tension and anxiety, a small area, such as an acupressure point along a vertical meridian line, could be addressed rather than attempting a complete urban redesign. Green space is prevalent in urban planning. However, an actual plan for the green space is often missing. Green space can mean a small strip of grass, or a few trees added as an afterthought. Applying other eastern principles, such as aromatherapy would be a progressive addition to the design phase. For example, if there is a lack of people using a public space where there is ample seating, adding a vertical garden with aromatic herbs may draw people to the area. Aromatherapy, or a fragrance garden, on a large scale could enhance individual experiences while reducing stress and anxiety. It also gives purpose to a vertical garden aside from aesthetics. Incorporating vespertine gardens (night blooming) would help understand that urban areas have enormous potential after sunset; and would also align with solar and lunar lighting during the design phase. Nocturnal plants are more fragrant and assist visually impaired individuals when combined with other sensory plantings. Using balance between day/night, light/dark can create enough stability to reduce tension and anxiety. Urban acupuncture is an intriguing starting point to reconsider conventional urban planning and design. It highlights that we are at a critical moment in time when all stakeholders can think about long term plans and how those plans will have a positive impact on mental and public health in urban centers.  Caixa Forum Museum employing concepts of urban acupuncture and aromatherapy to urban design. More details. About the author
|
Sanity and Urbanity:
|



 RSS Feed
RSS Feed